
Prostate Cancer
Introduction
Advances in care are offering more options to men who have prostate cancer. When found early, prostate cancer has one of the highest survival rates of any cancer. For advanced stages, a variety of treatments are available.
The Prostate Gland
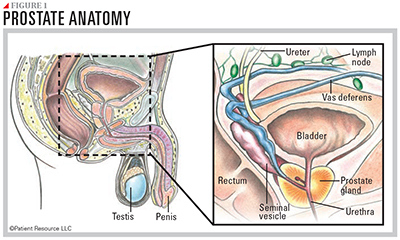
The prostate is a walnut-sized gland located behind the base of the penis, situated under the bladder and in front of the rectum (see Figure 1). It wraps around the urethra, the tube-like channel that carries urine and semen through the penis. The prostate makes seminal fluid, the liquid in semen that protects, supports and helps transport sperm out of the body.
As men age, their prostate tends to enlarge. This may result in symptoms such as problems with urination or sexual function, but an enlarged prostate does not mean you have cancer. Such enlargement with age is called benign prostatic hypertrophy (BPH). One of the symptoms is that the urethra becomes blocked, making it difficult to urinate. Although blockage of urine flow may occur because of prostate cancer, such symptoms are far more likely to be caused by BPH, which is not associated with a greater risk of developing prostate cancer.
It is important to be in tune with your body and be willing to talk with your medical team about any symptoms to determine what is causing them.
About Prostate Cancer
Cancer begins when healthy cells in the prostate change and grow out of control, forming a tumor.
Early-stage prostate cancer means the cancer is contained within the prostate and has not spread outside of the gland. Advanced stage prostate cancer has metastasized, or spread, beyond the prostate to other areas of the body. Metastasis occurs when cancer cells travel throughout the body via the bloodstream or the lymphatic system. The lymphatic system is the network of lymph nodes and vessels that are critical for your body to fight infections. Disease-fighting cells such as lymphocytes are carried in the clear fluid called lymph, which circulates throughout the body. Lymph nodes help filter the lymph fluid to remove germs and fight disease. They are found all over the body.
Seek a Second Opinion
Once you receive a prostate cancer diagnosis, consider getting a second opinion. Your care decisions may affect many areas of your life. You deserve to explore all your options.
Your urologist may have made the initial diagnosis, and while you may be very confident with that care team, you could benefit from talking with specialists who have extensive experience treating your type of prostate cancer. These may include a pathologist, medical oncologist, radiation oncologist or surgeon.
Getting a second opinion can be beneficial in the following situations:
- There is uncertainty surrounding your diagnosis.
- You want to feel more confident that you have chosen the best treatment plan.
- You would like to learn about other treatment strategies.
- You are not comfortable with your medical team’s communication style or with the treatment options you have been given.
- You have a rare or advanced form of prostate cancer.
- Your insurance company requires one.
Terms to Know
A cancer diagnosis comes with new vocabulary. It may help to familiarize yourself with some common terms.
First-line therapy is the first treatment given for a disease. It is often composed of a combination of treatments, such as surgery followed by hormone therapy, chemotherapy and/or radiation.
Local therapy is treatment that is directed to a specific organ or limited area of the body. For prostate cancer, local treatments include surgery and radiation therapy.
Metastasis is the spread of cancer cells from the place where they first formed to another part of the body.
Oncologist is a doctor who has special training in diagnosing and treating cancer.
Palliative care is given to improve the quality of life and help reduce pain in people who have a serious or life-threatening disease, such as cancer.
Recurrence is when cancer comes back, usually after a period of time during which it could not be detected.
Standard of care is treatment that is accepted by medical experts as a proper treatment for a certain type of disease and that is widely used by health care professionals.
Systemic therapy uses medication that travels through the bloodstream, reaching and affecting cells all over the body. Medications may be given intravenously (through an IV) into a vein or swallowed orally (a pill or capsule).
