Small Cell Lung Cancer
Staging
People who receive a cancer diagnosis are often asked about their stage. Though it is sometimes thought of as an indicator of how advanced the cancer is, it is much more. The staging process allows your medical team to learn more about your specific diagnosis and, in turn, provide you with a prognosis (outlook) and a treatment plan.
Your doctor collaborates with other medical professionals to learn about your cancer. They review the results of your physical examination, lab and imaging tests, and biopsies. They evaluate the size and location of the cancer and whether it has metastasized (spread) to nearby organs, tissues or lymph nodes, or to other parts of your body. The final step is for the doctor to stage your cancer using one or a combination of two staging systems.
The Veterans Administration Lung Study Group (VALSG) created the first staging system for SCLC. It separates SCLC into limited stage and extensive stage.
- Limited-stage SCLC is confined to one part of the chest, in just one part of the lung and in nearby lymph nodes.
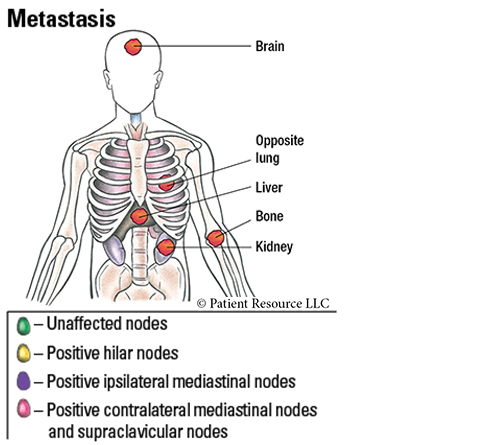
- Extensive-stage SCLC has spread to other parts of the body, such as the area between the lungs or the opposite lung, or outside of the chest, such as to the brain or bone.
In the American Joint Committee on Cancer’s (AJCC) and International Association for the Study of Lung Cancer’s TNM classification and staging system, the T category identifies the primary tumor’s size and location. The N category indicates whether lymph nodes show evidence of cancer cells. If so, the location of these lymph nodes is important because it shows how far the disease has progressed. The M category describes distant metastasis (spread), if any, that can be detected only by using a microscope.
Your T, N and M status are combined and assigned a number:
- Stages I and II are generally confined to the local area where the cancer is found, with or without nearby lymph node involvement. They are treated as early stage and are considered potentially curable; therefore, every effort should be made to render a cure for these diagnoses.
- Stage III is considered locally advanced, still confined to the chest but having spread to regional lymph nodes outside the lung in the mediastinum (area between the lungs).
- Stage IV is locally or regionally advanced disease that has spread to distant sites.
Some doctors combine the staging systems to enhance diagnosis and treatment planning.
- Limited-stage is considered to be Stages I to III of the AJCC TNM staging system, but Stage I SCLC is not common.
- Extensive-stage is considered to be Stage IV in the AJCC TNM staging system.
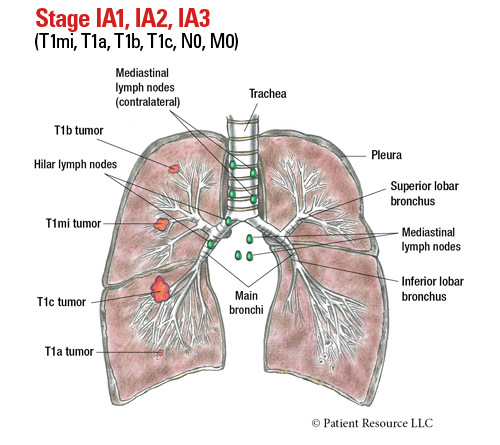
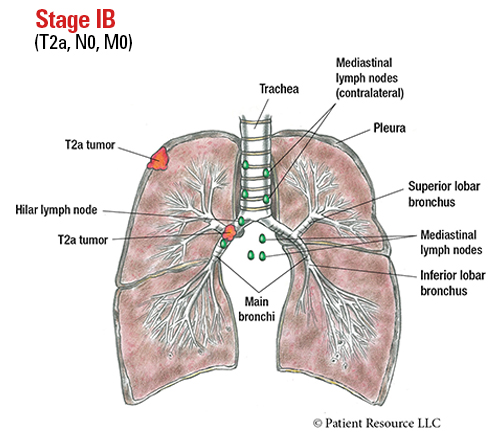
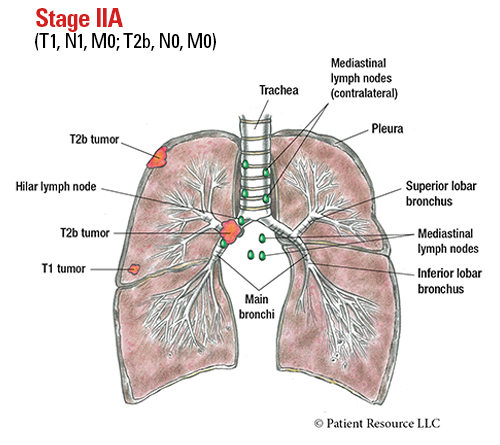
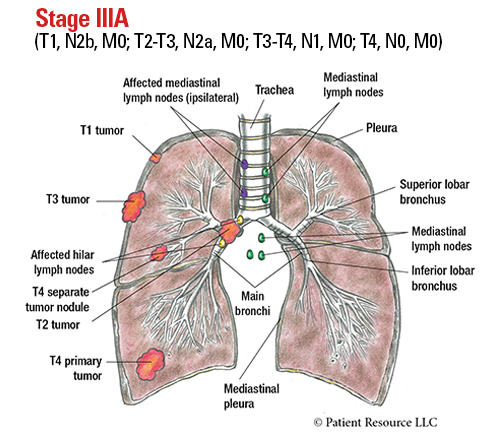
Sample AJCC staging illustrations show tumors on one side of the lungs. However, tumors may be present in any area of the lungs. These examples are not meant to represent the amount or placement of your tumors.
Table 1. AJCC TNM System for Classifying Lung Cancer
| Category | Definition |
| Tumor (T) | |
| TX |
Primary tumor cannot be assessed.
Includes tumors proven by the presence of malignant (cancerous) cells in sputum (mucus that has been coughed up) or bronchial washings (cells collected from inside the airways) but not visualized by imaging or bronchoscopy. |
| T0 | No evidence of primary tumor. |
| Tis |
Carcinoma in situ.
Squamous cell carcinoma in situ (SCIS). Adenocarcinoma in situ (AIS): adenocarcinoma with pure lepidic pattern (on the alveolar lining), not more than 3 cm in greatest dimension. |
| T1 | Tumor not more than 3 cm in greatest dimension, surrounded by lung or visceral pleura (membrane surrounding the lung), or in a lobar or more peripheral bronchux (i.e., not in the main bronchus). |
| T1mi | Minimally invasive adenocarcinoma: adenocarcinoma not more than 3 cm in greatest dimension with a predominantly lepidic pattern (on the alveolar lining) and not more than 5 mm invasion in greatest dimension. |
| T1a |
Tumor not more than 1 cm in greatest dimension.
OR Tumor of any size whose invasive component is limited to the bronchial wall and may extend proximal to the main bronchus, this is an uncommon superficial, spreading tumor. |
| T1b | Tumor more than 1 cm but not more than 2 cm in greatest dimension. |
| T1c | Tumor more than 2 cm but not more than 3 cm in greatest dimension. |
| T2 |
Tumor more than 3 cm but not more than 5 cm
OR Tumor not more than 4 cm with one or more of the following features: • Invades visceral pleura (membrane surrounding the lung. • Invades an adjacent lobe. • Involves main bronchus (up to but not including the carina) OR • Associated with atelectasis (collapse of part of the lung) or obstructive pneumonitis (inflammation of lung tissues) extending to the hilar regions, involving part of or the entire lung. |
| T2a |
Tumor more than 3 cm but not more than 4 cm in greatest dimension.
OR Tumor not more than 4 cm in greatest dimension with one or more of the following features: • Invades visceral pleura (membrane surrounding the lung). • Invades an adjacent lobe. • Involves main bronchus (up to but not including the carina) OR • Associated with atelectasis (collapse of part of the lung) or obstructive pneumonitis (inflammation of lung tissues) extending to the hilar regions, involving part of or the entire lung. |
| T2b |
Tumor more than 4 cm but not more than 5 cm in greatest dimension with or without any of the following features:
• Invades visceral pleura (membrane surrounding the lung).
• Invades an adjacent lobe. • Involves main bronchus (up to but not including the carina) OR • Associated with atelectasis (collapse of part of the lung) or obstructive pneumonitis (inflammation of lung tissues) extending to the hilar regions, involving part of or the entire lung. |
| T3 |
Tumor more than 5 cm but not more than 7 cm in greatest dimension
OR Tumor not more than 7 cm with one or more of the following features: • Invades parietal pleura (outer lung membrane) or chest wall • Invades pericardium, phrenic nerve or azygos vein Although these structures lie within the mediastinum, the degree of mediastinal penetration by the tumor needed to invade these structures is not counted as T4 • Invades thoracic nerve roots (i.e. T1, T2) or stellate ganglion • Separate tumor nodule(s) in teh same lobe as the primary |
| T4 |
Tumor more than 7 cm in greatest dimension
OR Tumor of any size with one or more of the following features: • Invades mediastinum (except structures listed in T3), thymus, trachea, carina, recurrent laryngeal nerve, vagus nerve, esophagus or diaphragm • Invades heart, great vessels (aorta, superior/inferior vena cava, intrapericardial pulmonary arteries/veins), supra-aortic arteries or brachiocephalic veins • Invades subclavian vessels, vertebral body, lamina, spinal canal, cervical nerve roots or brachial plexus (i.e., trunks, divisions, cords or terminal nerves) • Separate tumor nodule(s) in a different ipsilateral (on the same side) lobe than that of the primary |
| Node (N) | |
| NX | Regional lymph nodes cannot be assessed. |
| N0 | No tumor involvement of regional lymph node(s). |
| N1 | Tumor involvement of ipsilateral (on the same side) peribronchial and/or ipsilateral hilar and/or ipsilateral intrapulmonary lymph node station(s), including involvement by direct extension. |
| N2 | Tumor involvement of ipsilateral (on the same side) mediastinal nodal station(s) and/or subcarinal lymph node station. |
| N2a | Tumor involvement of a single ipsilateral (on the same side) mediastinal nodal station or of the subcarinal nodal station. |
| N2b | Tumor involvement of multiple ipsilateral (on the same side) mediastinal nodal stations with or without involvement of the subcarinal nodal station. |
| N3 | Tumor involvement of contralateral (on the opposite side) mediastinal, contralateral hilar, ipsilateral (on the same side) or contralateral scalene, or ipsilateral/contralateral supraclavicular lymph node station(s) (located above the collarbone). |
| Metastasis (M) | |
| M1 | Microscopic confirmation of distant metastasis. |
| M1a |
Microscopic confirmation of metastasis in pleural or pericardial nodules, and/or malignant pleural or pericardial effusions, and/or separate tumor nodule(s) in a contralateral (on the opposite side) lobe.
Note: Most pleural (pericardial) effusions with lung cancer are a result of the tumor. In a few patients, however, multiple microscopic examinations of pleural (pericardial) fluid are negative for tumor, and the fluid is non-bloody and not an exudate. If these elements and clinical judgment dictate that the effusion is not related to the tumor, the effusion should be excluded as a staging descriptor. |
| M1b | Microscopic confirmation of single extrathoracic metastasis in a single organ system (including involvement of a single non-regional node). |
| M1c | Microscopic confirmation of multiple extrathoracic metastases in a single or multiple organ system(s). |
| M1c1 |
Microscopic confirmation of multiple extrathoracic metastases in a single organ system.
Note: For example, the skeleton is considered one organ. Several metastases in a single bone or several metastases in several bones are classified as M1c1. |
| M1c2 | Microscopic confirmation of multiple extrathoracic metastases in multiple organ systems. |
Table 2. Stages of Lung Cancer
| Stage | TNM classifications |
| Occult carcinoma | TX, N0, M0 |
| 0 | Tis, N0, M0 |
| IA1 | T1mi-T1a, N0, M0 |
| IA2 | T1b, N0, M0 |
| IA3 | T1c, N0, M0 |
| IB | T2a, N0, M0 |
| IIA |
T2b, N0, M0
T1, N1, M0
|
| IIB |
T1, N2a, M0
T2a-T2b, N1, M0
T3, N0, M0
|
| IIIA |
T1, N2b, M0
T2-T3, N2a, M0
T3-T4, N1, M0
T4, N0, M0
|
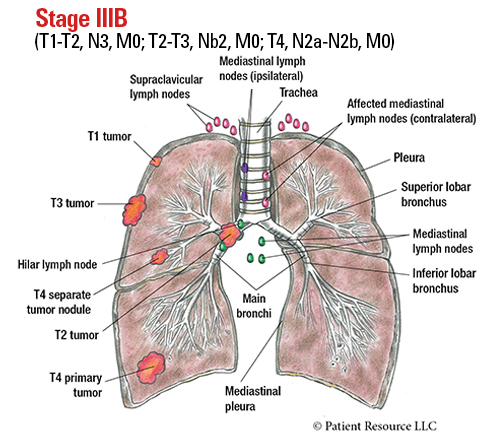
| IIIB |
T2-T3, N2b, M0
T4, N2a-N2b, M0
T1-2, N3, M0
|
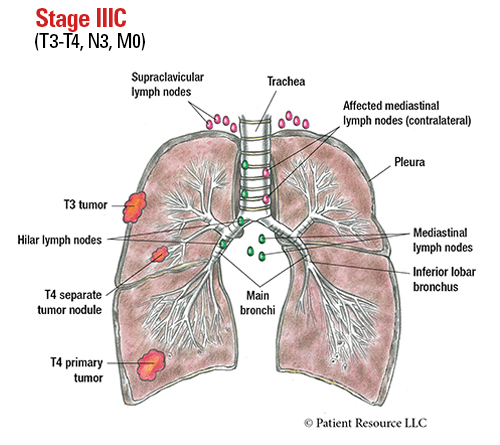
| IIIC |
T3-T4, N3, M0
|
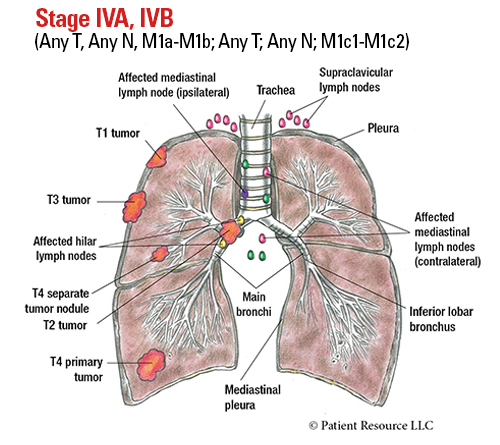
| IVA |
Any T, Any N, M1a-M1b
|
| IVB |
Any T, Any N, M1c1-M1c2
|
AJCC Illustrated Stages of Lung Cancer
KEY WORDS
Contralateral: on the opposite side as the primary tumor
Hilar lymph nodes: in the lungs, in the region where the bronchi, arteries, veins and nerves enter and exit the lungs
Ipsilateral: on the same side as the primary tumor
Mediastinal lymph nodes: between the lungs, in the part of the chest that lies between the sternum and the spinal column