Triple Negative Breast Cancer
Treatment Options
More people are living longer with triple negative breast cancer (TNBC) as a result of newly approved drug therapies. Although TNBC remains an aggressive disease that needs more treatment options, research is ongoing and new forms of treatment are being pursued. These advances offer hope for even better outcomes.
Your health care provider will consider many factors before recommending the best treatment options for you. Understanding the goal(s) of treatment, as well as being aware of the benefits and risks of each option, will help you be more prepared to make shared treatment decisions with your health care provider.
Fertility Preservation
Before making any treatment decisions, if possible, talk with your health care provider about how each option may affect your fertility. Depending on where you are in your life, this may be a challenging topic. You may be in the process of trying to become pregnant, or you may be years away from even thinking about it. Regardless, it is important to know up front that some treatments can cause temporary or permanent infertility.
A fertility specialist can explain your options for fertility preservation, the process of saving or protecting your eggs or reproductive tissue, to have biological children in the future. Options may include egg freezing (egg banking, egg cryopreservation or oocyte cryopreservation), embryo freezing (embryo banking or embryo cryopreservation), ovarian shielding (gonadal shielding), ovarian tissue freezing (ovarian tissue banking or ovarian tissue cryopreservation), ovarian transposition (oophoropexy) and radical trachelectomy (radical cervicectomy). Keep in mind that families are made in many ways, such as adoption and surrogacy.
Drug Therapy
Many patients now begin treatment with systemic drug therapy in order to reduce the size of the tumor before considering surgery (Figure 1). The drug therapy commonly includes chemotherapy and immunotherapy. This treatment may reduce or eliminate the need for surgery and/or radiation therapy, or determine if you may need to try a different drug combination. This allows for a more personalized approach to the unique characteristics and responsiveness of your individual tumor.
Chemotherapy is often necessary to treat TNBC. It is used to stop the growth of cancer cells either by killing them or preventing them from dividing and growing. Chemotherapy drugs are usually given in a regimen, which includes the drugs to be used, the dosage and the specific time period. In some cases of TNBC, chemotherapy may be given as a combination of two or three drugs together or one after the other.
Research has shown that TNBC may respond better to chemotherapy than to other types of breast cancer. Several chemotherapy drugs are available, and they may be given in combination with each other or sequentially (one after the other) over a specific period (usually three to six months). The chemotherapy regimens used most often are anthracycline-based or taxane-based.
Chemotherapy may be given before surgery (neoadjuvant therapy) or after surgery (adjuvant therapy). When given before surgery, it may be used to shrink a tumor so it can be more easily surgically removed or to shrink a large breast tumor to allow for a lumpectomy rather than a mastectomy. Neoadjuvant
chemotherapy is also often used in patients where cancerous axillary (armpit) lymph nodes are found at the time of initial breast cancer diagnosis. The pathology findings from the breast and lymph node tissue removed after neoadjuvant chemotherapy provide important clues regarding prognosis (outlook).
If the pathology report shows that the chemotherapy completely eliminated the cancer (called a complete pathologic response), this indicates that the chemotherapy regimen was very effective, and long-term survival rates are excellent — even with TNBCs. For TNBCs that have residual disease after neoadjuvant chemotherapy, recent research shows that additional medication, including immunotherapy, can improve outcomes.
Adjuvant chemotherapy is given to destroy cancer cells that may remain after surgery, some of which may be too small to be detected with laboratory testing or imaging studies. This can decrease the risk of recurrence in higher-risk patients and most patients with TNBC.
Chemotherapy may be given orally or intravenously through a vein in your arm. Many people have a port installed so they can receive the medicine without repeatedly being stuck with a needle or damaging their veins. A port is surgically inserted under the skin in the upper arm or chest area to gain easy access to veins. Once chemotherapy ends and you no longer have the need for easy access to your veins, the port is removed.
If your disease doesn’t respond as expected to one chemotherapy drug, your health care provider may recommend another. Researchers continue to study various chemotherapy combinations and the genetic makeup of tumors to determine which regimens work best against the specific characteristics of different tumor types.
Targeted therapy is a type of treatment that uses drugs or other substances to identify and attack specific types of cancer cells. The goal of targeted therapy is to slow the progression of disease. Unlike chemotherapy, which attacks healthy cells as well as cancer cells, targeted therapy either targets a cancer cell’s internal functions, receptors on the outside of the cell or the blood vessels that support the tumor. Normal cells (such as those that cause hair loss) are affected less.
Targeted therapy is a more recent addition to treatment options for people with TNBC. Two classes of targeted therapy are now available: poly (ADP-ribose) polymerase (PARP) inhibitors and antibody drug conjugates (ADC).
PARPs are approved for breast cancers with the BRCA1 or BRCA2 gene mutation. These drugs block cancer cells from repairing themselves, which causes them to die. Knowing whether you are a good candidate for this targeted therapy may require genetic testing to determine whether you have either of these two mutations.
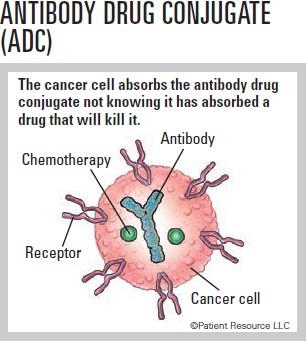
Antibody drug conjugates (ADC) are a monoclonal antibody or laboratory-made protein that targets specific tumor antigens found on cancer cells and is chemically linked to a chemotherapy drug. The antibody attaches to cancer cells so that the chemotherapy can be brought directly to the cancer cell, sparing most healthy cells. It gets swallowed by the tumor cell and breaks down inside the cell, releasing the chemotherapy drug, preventing growth signals and causing cell death.
Immunotherapy uses the body’s own immune system to recognize and attack cancer cells that have been hiding and targets them for destruction. Immune checkpoint inhibitors target the protein PD-1 (programmed cell death protein 1) found on immune cells and boost the immune system’s cancer-fighting response. It may be recommended if you have metastatic or recurrent TNBC or early-stage TNBC that is high risk.
In some cases, you may qualify for tumor-agnostic treatment. This is a new class of drug therapy that is approved to treat solid tumors anywhere in the body that meet specific criteria:
- Tumors are metastatic or unresectable (cannot be removed with surgery).
- The tumor must contain a greater than normal amount of molecular alterations.
- The cells must contain a mutation that prevents them from fixing errors that occur during duplication.
Surgery
Surgery may be the primary treatment for early stage TNBC but it is often used in combination with chemotherapy, immunotherapy and radiation therapy. Sometimes, drug therapy may be done prior to surgery.
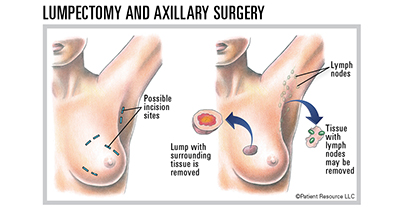
A lumpectomy is known as “breast-conserving treatment” because most of the breast is left intact. The surgeon removes only the tumor (lump) and a small amount of healthy tissue around the lump (see Figure 3, page 8). Lumpectomy can be done for most small tumors.
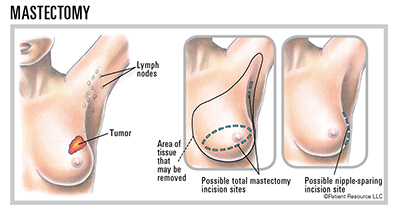
A mastectomy, which is surgery to remove the entire breast, is often done for large tumors, especially when they occur in a smaller breast. Some people with a small tumor may choose a mastectomy to ease their worry about cancer recurrence, and some choose this option as a way to potentially avoid radiation therapy. Your surgeon may recommend a mastectomy if you have a large tumor, multiple tumors in the breast or cancer that has spread to the skin, if you’ve already had breast cancer in the same breast or if you have a BRCA mutation.
Lymph node dissection is surgery to remove lymph nodes under the arm to examine them for cancer cells. Diagnosis and treatment of cancer in the lymph nodes is typically performed in addition to the primary surgery. After detection by X-ray or ultrasound, determining whether the cancer has spread to adjacent lymph nodes can be confirmed either from a needle biopsy or a “sentinel node” biopsy performed under anesthesia at the time of your breast surgery. If you do not have any bulky or obvious cancer-containing lymph nodes in your underarm, your surgeon can focus on removing only the few most important lymph nodes, called the sentinel lymph nodes. Sometimes a more extensive lymph node operation is required to control disease called an axillary lymph node dissection (see Figure 3, page 8). The axillary lymph node dissection can increase the risk for a problem called lymphedema, which is swelling of the arm. Even if you have bulky spread to the lymph nodes, a trial treatment with chemotherapy, often in combination with immunotherapy, may shrink the tumors so that radical surgery may not be necessary.
Breast reconstruction may be an option to consider after having a lumpectomy or mastectomy. Breast reconstructive surgery, which should be performed by an experienced plastic reconstructive surgeon, is typically started or even completed at the same time as a mastectomy but can happen later (within months or longer after the mastectomy). It may be done during or after a lumpectomy when the surgery will cause the affected breast to look significantly different in size or shape from the other after the tumor is removed. Even in this situation, the surgeon can move some of the adjacent breast tissue around to reduce the magnitude of any deformity.
Some patients are candidates for skin-sparing and nipple- and areola-sparing mastectomy. Reconstruction following mastectomy may be done in phases. What is important is to achieve symmetry of the breast, which can be a work in progress. In some cases, it may be necessary to perform a breast reduction on the opposite (normal) side in order to achieve symmetry. Remember that this is a “quality of life” issue and every woman has different desires about the degree of symmetry of their breasts that they want to achieve, even if this is simply to be able to wear your bra and bathing suits comfortably.
Different breast reconstruction techniques are available. They may involve the use of a breast implant or a flap of tissue (usually containing skin, fat, possibly muscle and blood vessels) from elsewhere in your body, or a combination of the two. The use of a tissue flap depends on the size of your breasts, your body type and preferences regarding appearance.
Prophylactic mastectomy reduces the risk of a new breast cancer but it does not completely eliminate the risk because microscopic amounts of breast tissue can remain hidden in the skin flaps or in the underarm fatty tissue after a mastectomy. Talk to your doctor about these potential options before deciding if prophylactic surgery is right for you.
Non-surgical options also exist. If you prefer not to have additional surgery or want the appearance of breasts while you are waiting to have reconstructive surgery later, you may want to consider a breast prosthesis.
Another option some women choose is to “go flat,” which means not having a breast prosthesis, enhancement or additional surgery.
Prophylactic surgery may be an option for people who have BRCA mutations and/or hereditary breast cancer. These women have a higher-than-average risk for developing new cancers in the contralateral (opposite) breast or in either breast if they’ve had a lumpectomy. BRCA mutations also increase the risk of developing a new cancer in the ovaries or the fallopian tubes. Women with one of these mutations may, therefore, choose to have prophylactic (preventive) removal of the ovaries and fallopian tubes or of both breasts as a precaution against potential future cancer.
Removal of the ovaries causes permanent infertility (the inability to have children) and premature menopause when performed on young women, as well as potential risks to bone and heart health. You should consult with a fertility expert if you are of child-bearing age and want to consider having children in the future.
Prophylactic mastectomy reduces the risk of a new breast cancer, but it does not completely eliminate it. Microscopic amounts of breast cancer can remain hidden in the skin flaps or in the underarm fatty tissue after a mastectomy. Nevertheless, the long-term results of large studies consistently demonstrate that risk-reduction surgery for preventing future breast cancer is a successful approach. Women should also consider other alternatives, such as chemoprevention and more intensive screening. Be informed and then choose what best fits your own risk tolerance and personal quality of life.
Radiation Therapy
The most common type of radiation therapy for TNBC is external-beam radiation therapy (EBRT). EBRT is delivered from an external machine. Internal radiation, or brachytherapy, may also be used either alone or in combination with EBRT. Brachytherapy involves placing radioactive seeds through a catheter into the breast to deliver radiation directly to the area where the tumor was removed.
Radiation therapy is almost always done after lumpectomy to destroy any cancer cells that may remain hidden in normal-appearing breast tissue. Research shows that women with a small tumor who have radiation therapy after a lumpectomy live as long as those who have a mastectomy. Radiation therapy is sometimes necessary after a mastectomy and is typically recommended for individuals at high risk for cancer recurrence on the chest wall, such as women with inflammatory breast cancer or women with cancer in several axillary lymph nodes. Radiation therapy is also used to control symptoms in some women with metastatic breast cancer and certain cases of bone or brain metastases.
Radiation treatments have complications and risks as well, including skin burning over the breast, shrinkage of the breast and potential long-term damage to the underlying bone or the heart. Some of the radiation effects have the potential to become disabling or disfiguring for many years after the treatment.
Clinical Trials
Clinical trials are an option you may want to explore as part of your treatment plan. Researchers and health care providers are learning more about the disease and how it responds to treatment, making clinical trials a valuable, potentially life-saving treatment option to consider. Clinical trials offer access to treatments that may work for some TNBCs. Ask your health care provider if any are available for you.
Dealing with Recurrence and Resistance
A recurrence is a term used when the breast cancer comes back in the same breast after initial treatment or in a distant site. Cancer returns when a few cancer cells remain undetected in the body. If this happens, the remaining cancer cells can multiply and become what is known as recurrent cancer.
Recurrent breast cancer may occur months or years after your initial treatment. If it recurs in the lymph nodes on the same side as the original breast cancer, it is called a regional recurrence. If it occurs in an organ in the body, it is a distant recurrence. If the cancer comes back outside of the breast, this regional or distant recurrence is also known as metastatic recurrence. All metastatic recurrences are considered advanced disease.
It is important to maintain your follow-up care to monitor for recurrence and track ongoing treatment, if applicable. Your health care provider will schedule regular exams at which you will be tested for signs of recurrence. Tell your health care provider if you notice any health changes at these exams or in between appointments.
A recurrence may be one of your biggest fears, but it is important to know that treatment options are available to you.
Being aware that cancer may return after your initial therapy is important, as is understanding resistance. Resistance is believed to develop when some cancer cells survive after being treated. The surviving cells recover and begin to grow and divide again, often with new genetic changes that the initial treatment is not designed to target.
Research is underway to understand how and why resistance develops and to find ways to prevent it or slow it down to extend the effectiveness of the original therapy. The most well-known treatment that can develop resistance is chemotherapy. However, it can also happen with targeted therapy and immunotherapy.
| Commonly Used Medications |
|
CHEMOTHERAPY
Combinations
|
|
TARGETED THERAPY
PARP inhibitors
|
As of 3/18/26
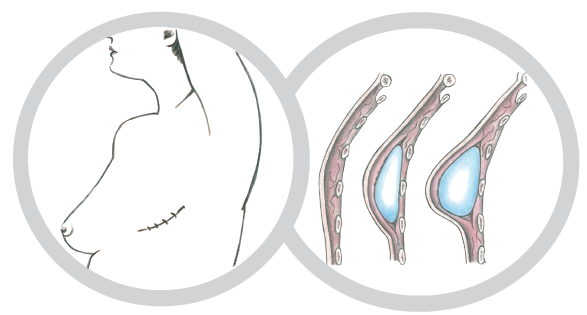
Reconstructive Techniques
With an Implant A breast implant filled with silicone gel or saline (salt water) may sometimes be placed following the mastectomy in a single operation referred to as immediate reconstruction. In delayed reconstruction, a tissue expander is inserted under the skin following the mastectomy to gradually stretch the skin and underlying tissue; an implant is then placed in a second surgery, often when treatment is completed.
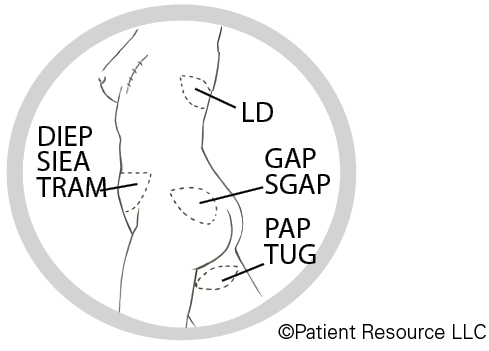
With a Tissue "FLAP" A tissue “flap” usually contains skin, fat, blood vessels and sometimes muscle. A pedicle flap remains attached to the body and is repositioned to the breast area with a muscle carrying the blood supply. A free flap is removed from the body along with blood vessels, which are then attached to the blood vessels in the breast area. Some types of flaps follow.
[DIEP] deep inferior epigastric perforator flap
[SIEA] superficial inferior epigastric artery flap
[TRAM] transverse rectus abdominis muscle flap
[LD] latissimus dorsi flap
[GAP] gluteal artery perforator flap (gluteal free flap)
[SGAP] superior gluteal artery perforator flap
[PAP] profunda artery perforator flap
[TUG] transverse upper gracilis flap